
“Within a matter of only seven months, we’ve more than halved the waiting time for a red flag hysteroscopy referral, and reduced waiting times for routine hysteroscopies too,” says Vicky Burns, Clinical Lead Nurse for Hysteroscopy at the Antrim Area & Causeway Hospital in Northern Ireland. Hysteroscopy can be used to detect uterine cancer, the fifth most common cancer among women in the UK, and faster investigation means greater survival rates.
Vicky is Northern Ireland’s first and only hysteroscopy nurse specialist. Her rare achievement was recognised this year when she was awarded RCN Northern Ireland Nurse of the Year for her huge impact on patient care and experience.

After completing postgraduate training and lobbying for the funding to set up a clinic in her trust, she’s now performing hysteroscopy as an outpatient procedure and helping to investigate and diagnose gynaecological cancers and other uterine conditions.
Before Vicky’s clinics opened, people were waiting 40 days for a red flag referral to hysteroscopy. Now, with her clinics reaching maximum capacity, the waiting time is down to only 14 days. “To see that paying off, that a role like this is doing what it’s supposed to, is fantastic,” Vicky says.
What is a hysteroscopy?
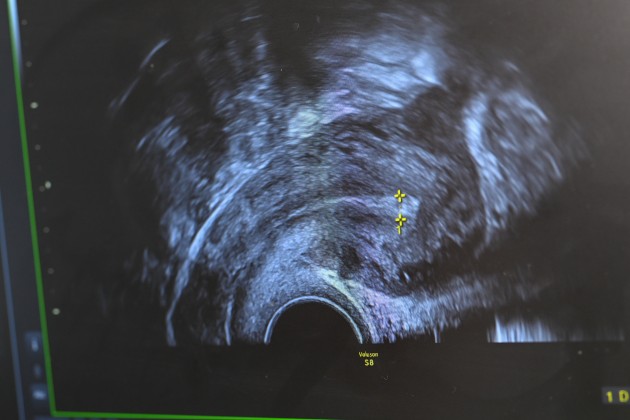
A hysteroscopy is a procedure used to examine the inside of the uterus. It’s carried out using a hysteroscope – a narrow telescope with a light and camera at the end. It is inserted into the uterus, via the vagina and cervix. Images from the camera are then analysed on screen.
Hysteroscopy can usually be carried out on an outpatient basis (if this is the patient’s preference), with the procedure itself taking between 5—10 minutes per patient, depending on what is being investigated or treated.
In previous years, before it was an outpatient procedure, hysteroscopy was performed in theatre under anaesthetic. Vicky’s team receives 60 to 90 referrals per week – “We wouldn’t have the theatre space to meet that demand.”
The main red flag symptom investigated by Vicky is abnormal uterine bleeding. “The majority of our workload will be post-menopausal bleeding. We know that, depending on risk factors, around 1 in 10 women with post-menopausal bleeding can have cancerous cells in their uterus. Uterine cancer is one of the most common cancers among females in Northern Ireland. Primarily, that's why patients are attending our clinics.”

As a student nurse, one of Vicky’s final placements was on a gynaecology ward, where she took up a band 5 post. She progressed to deputy ward sister and in 2019, an opportunity arose to train in hysteroscopy. Vicky was already trained as an ultrasound scanner, which is generally carried out before a hysteroscopy, so she had the perfect grounding. After periods training for the PGCert in Bradford, interrupted by the global pandemic, she completed the training in 2021.
Now, she runs 5 clinics, 3 in Antrim Hospital and 2 in Causeway Hospital. When a patient reports symptoms such as unexplained uterine bleeding, Vicky and team will investigate.
Why would a hysteroscopy be carried out?
- To investigate symptoms such as heavy periods, irregular bleeding, post-coital bleeding, postmenopausal bleeding.
- To diagnosis non-cancerous growths in the uterus, such as fibroids and polyps.
- To investigate the causes of repeated miscarriage or difficulty conceiving.
- To treat issues, for example by removing fibroids and polyps, or implanting an intrauterine device.
“We would first do a trans-vaginal scan. Based on that, if the lining of the womb is thickened we need to do a hysteroscopy,” Vicky explains. “A hysteroscope is a camera that we insert in through the vagina. We use a vaginoscopic approach, where we don’t insert speculums, as this method is much more tolerable to the patients. We traverse through the vagina to find the cervix and insert the camera through the cervix and into the womb.”

The hysteroscope also helps to open up the uterus. “The walls of the womb sit flat. As we enter the uterine cavity through the cervix, a distension medium of normal saline comes out the end of the camera and that will open up the uterine cavity so we can see the architecture and structures of the uterus. We pass some fine little biopsy forceps down the channel and take biopsies from the inside of the lining of the womb, which we send to the lab for analysis.”
The procedure can also be used to remove polyps and fibroids from the uterus. Other patients may be fitted with an intrauterine device – as part of hormone replacement therapy in menopausal women, to help with heavy menstrual bleeding, or to treat endometrial hyperplasia, a pre-cancer stage. “Hysteroscopy is a diagnostic procedure but it’s also a preventative and curative tool,” Vicky says.

While Vicky is the first nurse hysteroscopist in Northern Ireland, there are a handful of people in the role elsewhere in the UK. But there could be more. Training more specialist nurses in this role would be good for patients, Vicky says. “Nurses provide 24-hour care, and I have done that for 16 years, supporting people through their very worst and delivering bad news. You are there through the most intimate and fragile and devastating times for a woman and that pays off in the care you provide in a clinic like this.”
The majority of nursing staff are still women, and Vicky says her patients have commented on the comfort of being treated by an all-woman team in her hysteroscopy clinics. “It can be such an intimate and embarrassing procedure for a lady,” she says. “When they come in here and see it’s all ladies, you can see them thinking: ‘Oh thank goodness’.”

Now, Vicky is also training to become competent in colposcopy, so she can provide an integrated service across uterine and cervical procedures. She encourages others with an interest in this area of nursing to start conversations about how a hysteroscopy clinic could work in their trust. Vicky advises to research training opportunities and get buy-in from consultants and managers. “If you’ve got a good gynae grounding and rationale and training behind you, then you will find it so interesting,” she says.
The role is incredibly rewarding. “I love going to work and learning something new every day,” Vicky says. “I love being with the patients. A tedious day for me is one where I’m sitting in the office doing my admin, which is very necessary, but I’d rather be out in the clinic with patients and my colleagues having a yarn and a chat.”
When Vicky started out in gynaecology, she was told that, as a nurse, there was nowhere to go. She’s proven the naysayers wrong. “There’s continuity of care. I’m giving patients results, and if they need further treatment they’re coming back to the gynae ward beside where my clinics are based. I’m seeing them through the majority of their clinical pathway, it’s a familiar face, they know they’re going to be well looked after.”
It’s vital that patients feel comfortable reporting their symptoms and having the procedure. “We don’t really talk about it, irregular bleeding can be embarrassing. We need to normalise that these things can go wrong and they’re very, very common – which is reflected in how many referrals we have,” Vicky says.

“We know that early detection of uterine cancer has better outcomes. The earlier you're seen, the earlier it’s diagnosed, your chance of survival will be greater.”
Find out more
- Read about the RCN Women’s Health Forum and find out how to join here.
- Find resources for nurse hysteroscopists on the British Society for Genealogical Endoscopy.
- Visit RCN Learn to find out more about gynaecological cancers.





